Blood Sugar and Weight Gain: How Insulin Resistance Sabotages Your Weight Loss (2026 Complete Science Guide)
Why do some people gain weight eating 1,400 calories while others stay lean eating 3,000? The answer often lies in insulin resistance — the blood sugar dysfunction that locks fat cells shut regardless of caloric deficit. Here's the complete science.
The Weight Loss Mystery Most Doctors Don't Fully Explain
If you've ever followed a diet faithfully, counted calories religiously, and still couldn't lose weight — or if you've watched friends eat significantly more than you while staying lean without apparent effort — you may have encountered one of the most frustrating aspects of modern metabolic medicine: the blood sugar-weight connection.
The dominant weight loss paradigm — "eat less, move more" — is not wrong, but it's dangerously incomplete. It fails to account for the hormonal environment that determines how readily your body accesses its stored fat. And the single most important hormonal factor governing fat cell accessibility is insulin.
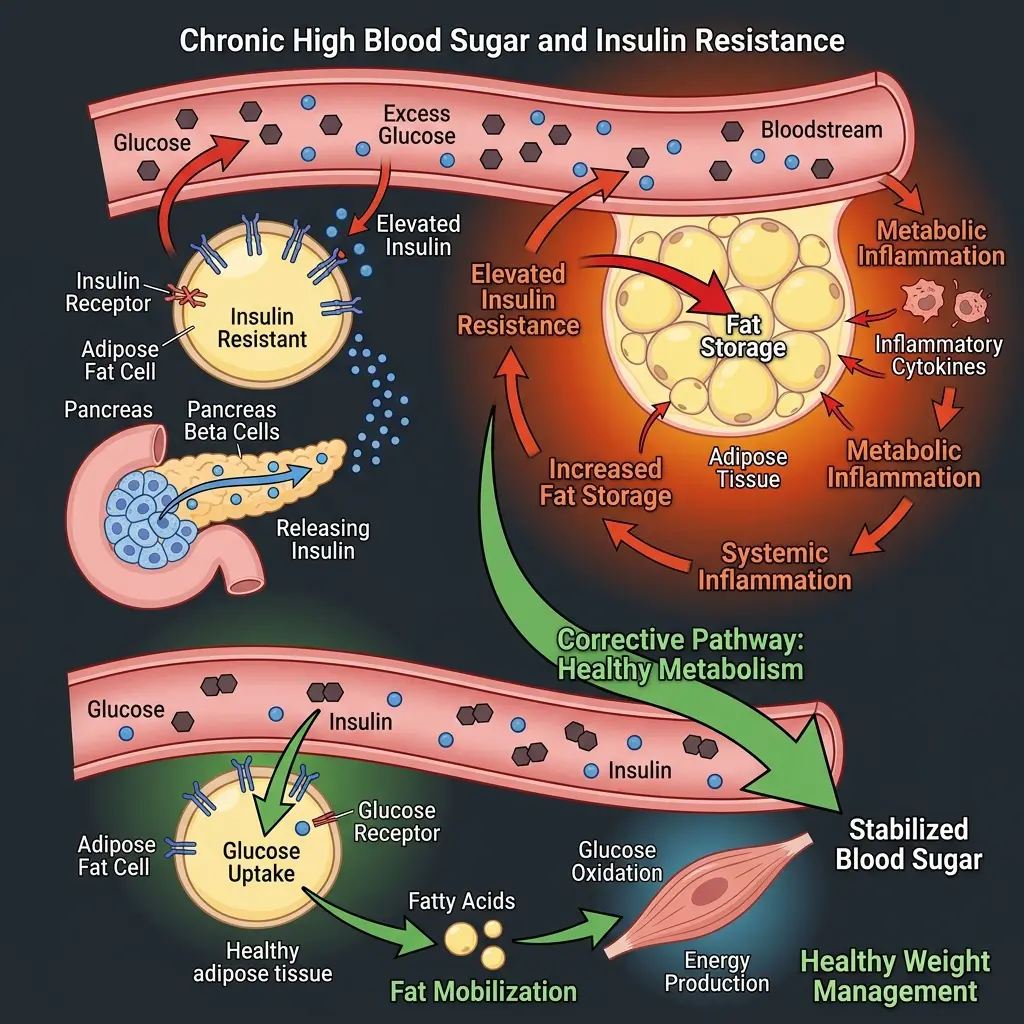
Insulin: The Most Powerful Metabolic Hormone You Might Not Be Managing
Insulin is secreted by pancreatic beta cells in response to blood glucose elevation. Its canonical role: stimulating glucose uptake in muscle, liver, and adipose tissue. But insulin has two additional actions that profoundly affect body weight:
- Inhibition of lipolysis: Insulin directly inhibits hormone-sensitive lipase (HSL) — the primary enzyme responsible for breaking down stored triglycerides in fat cells into free fatty acids for circulation and oxidation. Even moderate insulin elevation (well within the "normal" range post-meal) substantially suppresses fat mobilization. This means: while insulin is elevated after eating, you physiologically cannot access stored fat for energy.
- Promotion of lipogenesis: Insulin stimulates fatty acid synthesis in the liver (through activation of SREBP-1c and ChREBP transcription factors) and promotes de novo lipogenesis — the conversion of excess glucose into triglycerides that are deposited in fat cells. High-carbohydrate, high-glycemic diets therefore promote fat storage through insulin even in individuals who are not diabetic.
In a healthy metabolic state, insulin rises briefly after meals then falls as glucose is cleared — creating a "window" of lower insulin during which fat oxidation can proceed. In insulin-resistant individuals, baseline insulin remains chronically elevated, this window narrows or closes, and fat cells stay locked in storage mode.
The Insulin Resistance Cycle: How Being Mildly Overweight Makes Losing Weight Harder
Insulin resistance creates a self-reinforcing metabolic trap:
- Excess adipose tissue (particularly visceral fat) releases inflammatory cytokines (TNF-α, IL-6, resistin) that impair insulin receptor signaling in muscle and liver
- Impaired insulin signaling → pancreas compensates by secreting more insulin → hyperinsulinemia
- Chronic hyperinsulinemia → sustained HSL inhibition → fat cells remain locked → weight maintenance or gain
- Caloric restriction in this state produces muscle protein catabolism preferentially (body uses available amino acids for gluconeogenesis) rather than fat mobilization → unfavorable body composition changes despite weight loss on the scale
- The subjective experience: chronically fatigued, experiencing intense carbohydrate cravings (from reactive hypoglycemia), and not losing fat despite restriction → diet abandonment → weight regain
This cycle explains why standard caloric restriction is genuinely less effective in insulin-resistant individuals — a clinical finding confirmed by multiple RCTs showing that low-glycemic interventions (that reduce insulin secretion) produce superior fat loss vs. isocaloric high-glycemic diets even at identical caloric intake.
The Glucose-Craving Cycle: Why Blood Sugar Instability Drives Overeating
Postprandial glucose curves have a direct causal relationship with appetite and food choice over the following hours:
- The glucose spike: High glycemic index foods cause rapid glucose elevation → brain registers abundant energy → brief satiety
- The insulin overshoot: Insulin is secreted in anticipation of the glucose spike — in insulin-resistant individuals, more insulin is released than needed
- Reactive hypoglycemia: The insulin overshoot drives glucose below baseline → brain glucose shortage → aggressive hunger signals, particularly for fast-acting carbohydrates → "willpower problem" is actually a biology problem
- Cravings reinforcement: The dopamine reward of glucose correction from sweet foods reinforces the behavioral craving cycle — making high-glycemic food preferences increasingly difficult to resist
This mechanism explains why simply "eating less" fails for many people — they are fighting a neurobiological drive produced by their own glucose instability. Flattening the postprandial glucose curve (through lower-glycemic eating, meal sequencing, or targeted supplementation) addresses the biological driver of overeating rather than expecting willpower to override biochemistry.
Who Is Most Likely to Have Insulin Resistance?
Insulin resistance exists on a spectrum — full type 2 diabetes is the clinical endpoint of decades of progressive insulin resistance. But the subclinical stages (pre-diabetes and metabolic syndrome) affect an estimated 88 million Americans — 34% of the adult population — and the majority are unaware of their status.
Risk factors for subclinical insulin resistance:
- Central adiposity (waist circumference >35" women, >40" men)
- History of gestational diabetes or PCOS
- Strong family history of type 2 diabetes
- Chronic poor sleep quality (each week of poor sleep measurably increases insulin resistance)
- Sedentary lifestyle — skeletal muscle is the primary site of insulin-mediated glucose disposal; muscle loss worsens insulin sensitivity
- Diet high in refined carbohydrates and low in fiber
- Chronic psychological stress (cortisol antagonizes insulin signaling)
- Certain medications including corticosteroids, antipsychotics, and some blood pressure medications
How to Tell If Blood Sugar May Be Behind Your Weight Issues
These patterns suggest blood sugar instability may be a contributing factor:
- Energy "crashes" 2-3 hours after meals (reactive hypoglycemia)
- Intense cravings for sweets or carbohydrates, especially mid-afternoon or after dinner
- Feeling instantly hungry after a large meal
- Brain fog that improves after eating carbohydrates
- Difficulty losing body fat despite caloric restriction (particularly around the abdomen)
- Fasting glucose between 100-125 mg/dL (pre-diabetic range)
- HbA1c between 5.7-6.4% (pre-diabetic range)
- Significant energy difference between days you eat carbohydrates vs. days you don't
Evidence-Based Strategies to Break the Blood Sugar-Weight Cycle
1. Meal Sequencing
The order in which food categories are eaten significantly affects postprandial glucose response. Eating vegetables and protein BEFORE carbohydrates reduces the glucose spike from the same meal by approximately 30-40% (multiple RCTs from Cornell Medical). Mechanism: dietary fiber from vegetables slows gastric emptying and coats the intestinal brush border; pre-meal protein triggers GLP-1 and GIP secretion → pre-emptive insulin response → mitigated glucose spike.
2. Post-Meal Walking (10 minutes)
Skeletal muscle contraction activates GLUT4 translocation to cell membranes independently of insulin — providing a glucose disposal mechanism that bypasses insulin resistance. A 10-minute walk after eating reduces postprandial glucose by approximately 25-30% vs. sitting, with minimal cardiovascular stress. This is the most immediately actionable blood sugar management strategy available without supplementation.
3. Vinegar and Acidic Foods Pre-Meal
Acetic acid (from apple cider vinegar or white vinegar) taken before high-carbohydrate meals reduces postprandial glucose by approximately 34% (confirmed in multiple small RCTs). Mechanism: acetic acid inhibits amylase and glucosidase activity, slowing starch digestion and glucose absorption.
4. Targeted Blood Sugar Supplementation
Several botanicals and mineral compounds have Level-A evidence for improving insulin sensitivity and reducing postprandial glucose spikes:
- Berberine: AMPK activation comparable to metformin — the most clinically validated natural insulin sensitizer
- Gymnema Sylvestre: Intestinal glucose absorption inhibition + sweet receptor blocking for craving control
- Banaba leaf (corosolic acid): GLUT4 translocation independent of insulin — bypasses insulin resistance
- Alpha Lipoic Acid: Oxidative stress reduction + AMPK activation
- Cinnamon: Insulin mimetic procyanidins acting on insulin receptors
- White Mulberry DNJ: Glucosidase inhibition comparable to prescription acarbose
Products like Ignitra that combine multiple glucose-regulating compounds with educational materials (like the included Blood Sugar Blueprint) represent the most comprehensive approach to addressing blood sugar-driven weight resistance from a supplementation perspective.
Conclusion: The Blood Sugar Lens Changes Everything
For the estimated 30-40% of the adult population with some degree of insulin resistance, the conventional "eat less, exercise more" framework is not wrong — but it's insufficient. It treats weight as a pure energy balance problem while ignoring the hormonal environment that determines how effectively the body can access its stored fuel.
Adding blood sugar management as a foundational layer to any weight loss strategy — through meal sequencing, post-meal activity, glycemic food choices, and targeted supplementation — addresses the root metabolic cause rather than fighting an increasingly futile battle against biological drives created by glucose instability.